Young adults with SCD are at risk
While survival into adulthood has increased to >95% as a result of newborn screening and disease-modifying therapies, young adults remain at risk.
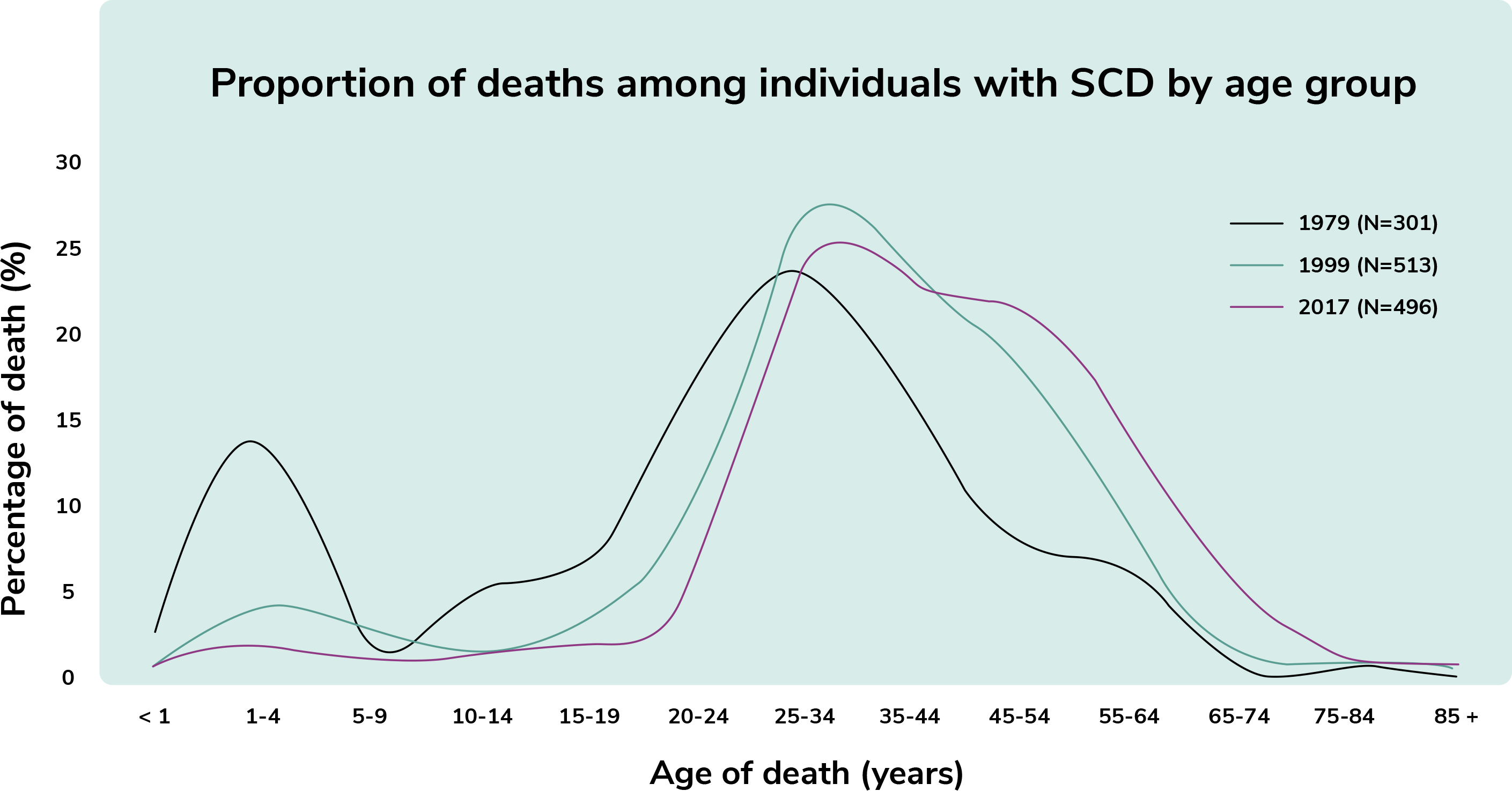
Recent data shows a sharp increase in mortality for people with SCD in their early 20’s. Adults with SCD also continue to die an average of 20 years earlier than race-matched counterparts.
People with SCD age 18-30 had the highest number of visits to the emergency department with an average of 4.8 visits per year and 41.1% were re-hospitalized within 30 days of visiting the hospital.
A rise in mortality occurs in the early adult years, coinciding with the period in which people transition from pediatric to adult care. This time is also associated with an increase in acute care utilization and disease severity.
The transition period from pediatric to adult care has critical gaps
The period of transition from pediatric to adult care is of critical importance to youth with SCD, however this is often when people meet with significant challenges. A combination of factors contribute to deterioration of health during this time.
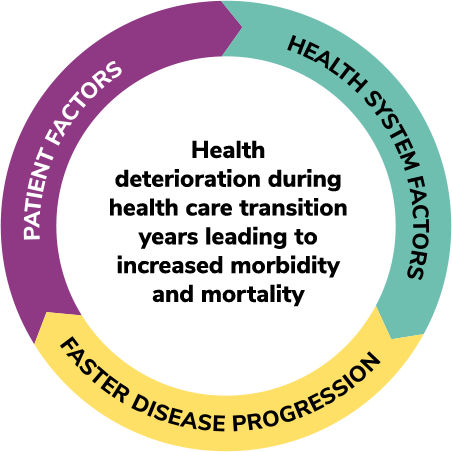
Lack of trained clinicians for adults with SCD is made worse by the progressive nature of the disease and cumulative damage as people age which includes:
- Bone damage
- Chronic pain
- Cognitive dysfunction
- Kidney disease
- Pulmonary hypertension
- Skin ulcers
Adolescents and young adults with SCD reported depression rates as high as 45% among adolescents and 27.6% in adults
SCD-related pain is real, and so is health-related stigma
SCD is characterized by red blood cells that assume a curved or “sickle” shape which causes them to stick to the walls of blood vessels leading to painful clotting withing capillaries and small vessels. This causes pain, tissue death and eventually anemia and end-organ conditions. These “pain episodes” are unpredictable and lead to feelings of inadequacy regarding their care due to health-related stigma.
- Numbness
- Aches
- Parasthesia
- Fatigue
- Jaundice of sclera
- Nausea
- Vomiting
- Change of appetite
- Joint stiffness
- Aches progress gradually to maximum pain
- Individuals will have decreased activity
- May also begin to have fear and anxiety about seeking care
- Duration of this phase can vary
- Phase when most individuals seek emergency care
- Pain is at its peak (it is steady and persistent)
- No relief from home medication
- Aches have progressed and joints may now be swollen and stiff
- Possible fever
- Lasts 4–6 days and often requires hospitalization
- Phase can be referred to as the resolving, recovery, or post-crisis phase
- Acute painful crisis is over
- Pain is now at a tolerable level
- Lasts 1–2 days and is usually when individual is discharged from the hospital
If adults with SCD present for treatment during the 2-4 day period of low pain intensity pre-crisis, they may avoid the need for aggressive pain management and hospitalization and have their pre-crisis pain adequately addressed.
What is health-related stigma?
Stigmatization when transitioning from pediatric to adult care
Young adults frequently face stigma as they transition out of pediatric care.
Without adequate preparation and support, they can become marginalized within the adult healthcare system, particularly when seeking treatment for acute pain.
Up to 80% of adults with SCD avoid the healthcare system and try to manage their pain at home
When young African American adults with SCD seek acute care, they are often questioned by healthcare providers unfamiliar with pain crisis who label them as “manipulators”.
When they request medications, this is often seen as “drug-seeking” behavior.
Currently adults with SCD who present in emergency departments with an acute pain episode may:
- Wait an average of 90 minutes to be given their first analgesic
- Face racial stereotyping
- Experience problematic physician communication
- Receive little SCD or acute pain education
Advocating for your care
The earlier treatment is initiated, the better the outcome is for people presenting with pain crisis.
Emergency room visits can be avoided or optimized when people with SCD:

Present earlier to a primary care setting that provides both medical and psychological support to identify and prevent severe crisis

Communicate key information to healthcare providers in the emergency room to help them identify them as well-informed, credible individuals presenting in the prodromal phase of an SCD crisis
Know what information healthcare providers need and how to communicate it in a positive manner