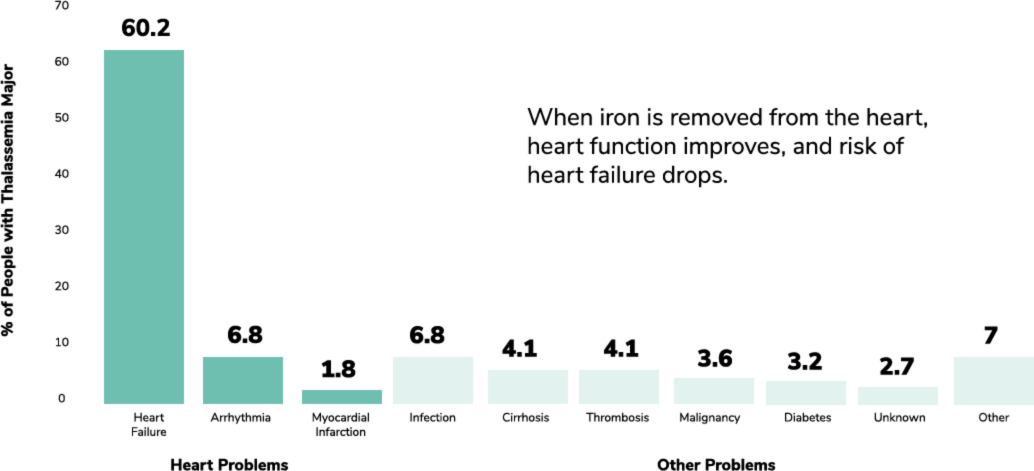
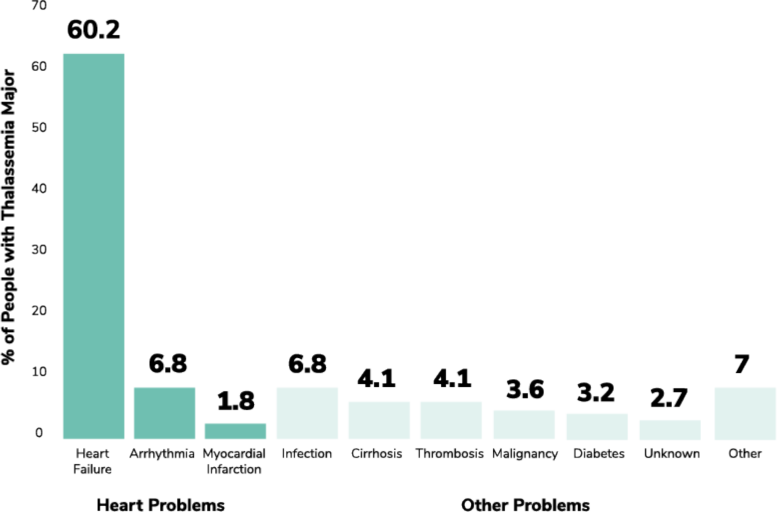
As iron continues to build up in the body, complications happen more often
About 70%
of deaths in
Despite improvements in care, cardiac iron overload is the leading cause of death among people with transfusion-dependent thalassemia
Don’t forget your other organs!
Careful monitoring of liver and kidney function is important to prevent further damage to the organs. Talk to your doctor and ensure you are on an appropriate iron chelator at the right dosing level that doesn’t impact your kidneys or liver.
The only way to know if your iron chelator is working is to have your iron levels checked regularly
Iron chelation needs to be adjusted regularly or even switched depending on your iron level, weight, and tolerance to side effects
| Lowering serum ferritin and liver iron concentration are not enough. Reducing cardiac iron is the priority in thalassemia. | ||
|---|---|---|
| Parameter | Target | Recommended monitoring |
| <1,000 ng/mL | Monthly | |
| >20 milliseconds (ms) | Yearly (or every 6 months if your T2* is <10 ms) | |
| 2-5 mg/g dry weight | Yearly | |
† MRI = magnetic resonance imaging