As iron continues to build up in the body, complications happen more often
60-70%
of deaths in
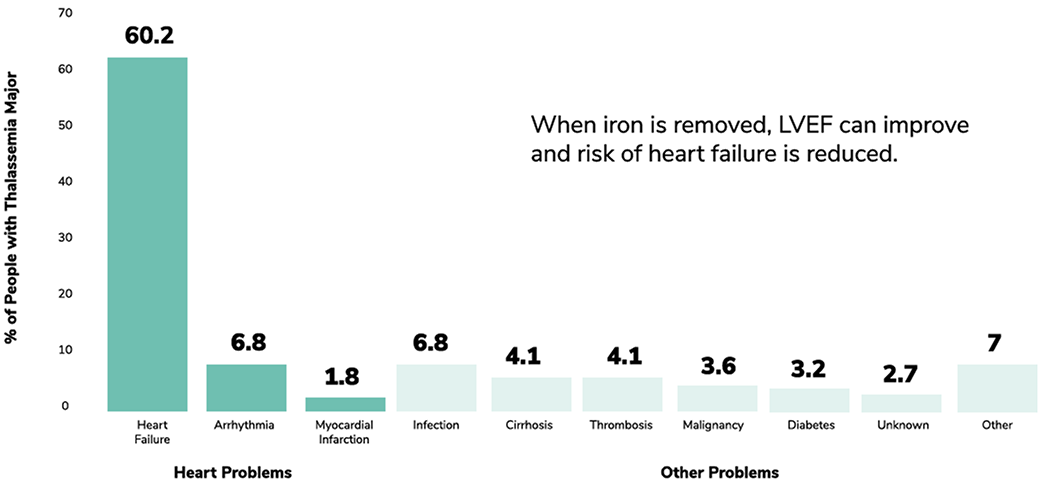
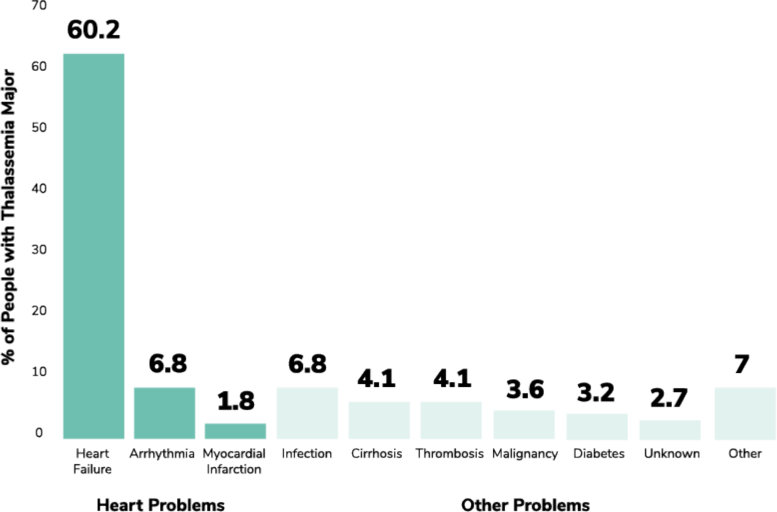
Causes of death in thalassemia patients until the late 1990s
When iron is removed, LVEF can improve, and risk of heart failure is reduced.
Consider renal/hepatic toxicity
Regular monitoring of both renal and hepatic toxicity can help optimize chelation and ensure patients are on an appropriate chelator.
The only way to know if your patients’ iron chelator is working is to have their iron levels checked regularly
Iron chelation needs to be adjusted regularly or even switched depending on iron level, weight, and tolerance to side effects
| Thalassemia treatment guidelines support regular monitoring of serum ferritin, and cardiac and liver MRI T2* | ||
|---|---|---|
| Parameter | Target | Recommended monitoring |
| Serum ferritin | <1,000 ng/mL | Monthly |
| Cardiac MRI T2* | >20 ms | Annually (Or every 6 months for those patients with T2* <10 ms) |
| Liver iron concentration (LIC) | 2-5 mg/g dry weight | Annually |